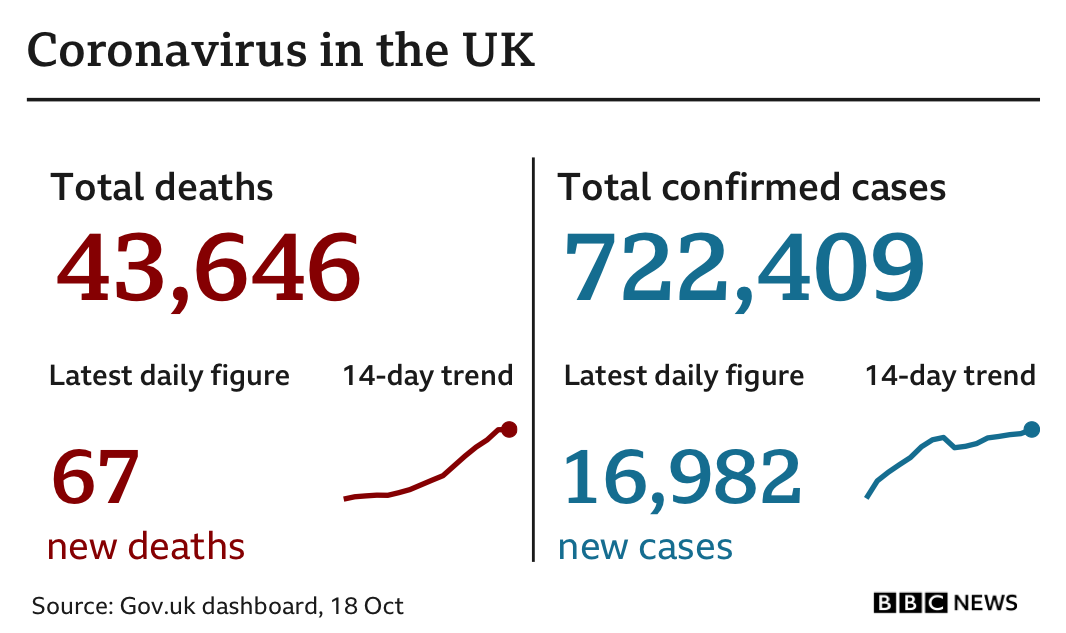
What needs to be looked at is the total deaths. They have fallen weekly over 80% since the end of July even though cases have increased. That shows a successful outcome if deaths decrease, because the cases will eventually come under control with the vaccine.
Also, why just the last 4 months? Look at the cases for the whole period from Mar to Oct (7 months) and I am sure more blue states would be in there (eg.NY, NJ,PE,MI,RI,MA,VT,OR,WA) This is just cherry picking a period of time to suit the writer's agenda IMO.
Again - why total deaths? Per capita deaths is what you want to look at. Total deaths isn't just cherry picking, it's meaningless unless you know the total population from which the deaths are coming.
Since deaths are reported by political jurisdictions that vary in size, it's virtually meaningless to compare total numbers from, say, India to those of Andorra.
Further, the next step is to locate the earliest death(s) per jurisdiction and then count the days out from that point (initial incidence date). Not every jurisdiction got CoVid at the same time. North Dakota, for example, doesn't appear in the top 15 per capita states for CoVid cases or deaths until almost exactly 2 months after Sturgis - because before that, they had almost no deaths.
Early on in the pandemic, major newspapers did employ techs to provide those graphs, but it has now grown too time consuming and public interest is waning, so we lost any ready ability to look at the data in that manner. Instead, most of us have to choose an arbitrary starting point for a series of comparison points.
It still says something way more than using "total deaths per jurisdiction."
For example, France's new cases as of yesterday were over 30,000 (but with a population slightly less than 1/5th of that of the US - so it would be like the US having 150,000 cases or a little more!)
UK has about 17,000 new cases today, with a population of almost exactly 1/5th of the US - so that would be like the US having 85,000.
If we look at
total cases per capita (Worldometers uses per million, move one decimal point to compare to other data sources that use per 100,000), then North Dakota has the most cases of all the states, over all periods of time, not New York, California, or New Jersey"
1. North Dakota
2. Louisiana
3. South Dakota
4. Mississippi
5. Alabama
6. Florida
7. Iowa
8. Tennessee
9. Arkansas
10. Georgia
11. South Carolina
12. Arizona
13. Texas
14. Nebraska
15. Idaho
Seeing a pattern? We're now getting into states that are more ranged around the average deaths per capita in the US. Since you were trying to argue a point about politics, those are
all red states.
Further, many of these states had their first infections well after the states you mentioned - but you decided not to do it per capita, which to me, is just raw data. We cannot compare the US to Andorra merely by total cases - or North Dakota to California.
California has 40 million people. North Dakota has only 762,061/
California is over 40X bigger in terms of sample size. And comes in 30 out of 50 states in terms of the number of people who have been diagnosed with CoVid - California also has a good testing regimen and has had CoVid cases from February onward. Check out the testing rates for each of those states listed above - you'll see a pattern there too.
21. New York
24. New Jersey
30. California
34. Massachusetts
The charts you are trying to argue with aren't using total numbers of cases - but per capita cases, as that's the only valid technique of comparison. This same method is use throughout science for comparison.